检验医学 ›› 2020, Vol. 35 ›› Issue (7): 721-725.DOI: 10.3969/j.issn.1673-8640.2020.07.021
杭晨1, 黄飚2, 彭海霞1, 韦欣1, 徐伟红1, 盛慧明1, 李宁丽3
HANG Chen1, HUANG Biao2, PENG Haixia1, WEI Xin1, XU Weihong1, SHENG Huiming1, LI Ningli3
摘要:
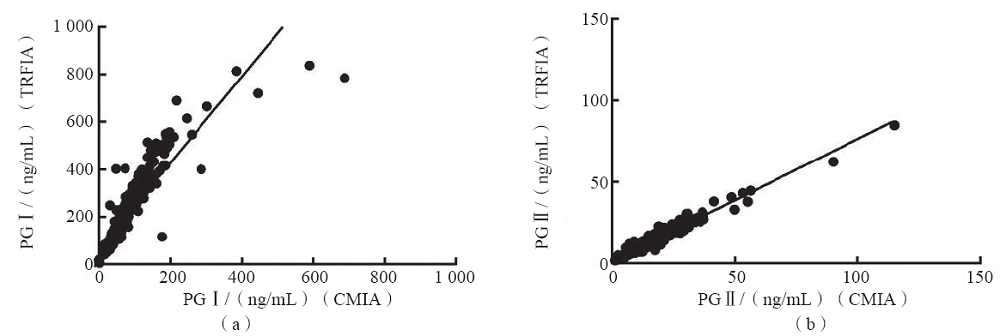
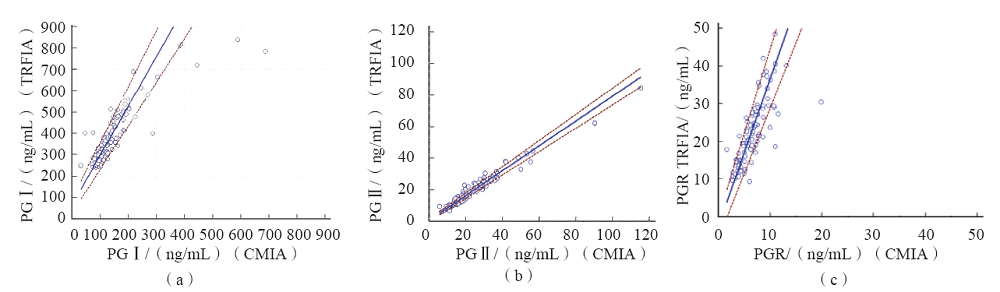
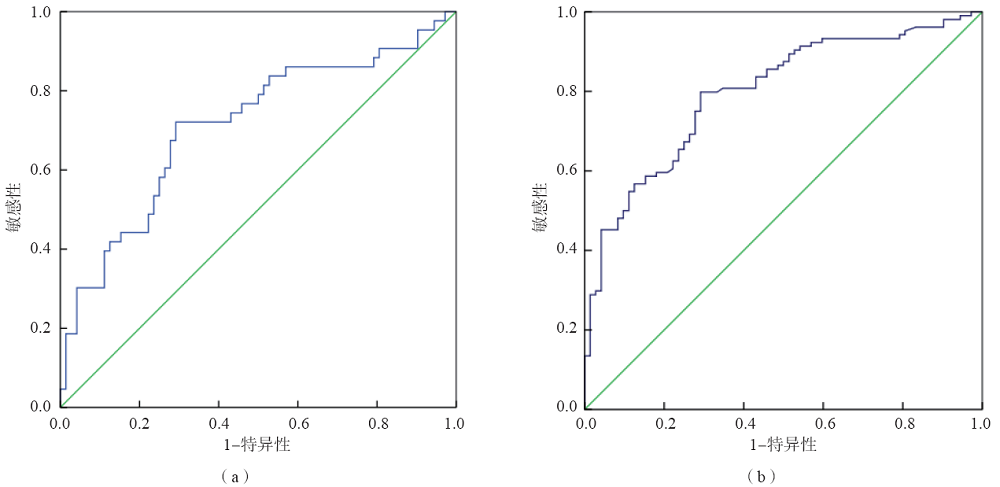
目的 探讨时间分辨荧光分析法(TRFIA)检测血浆胃蛋白酶原(PG)Ⅰ、PGⅡ和胃蛋白酶原Ⅰ/胃蛋白酶原Ⅱ比值(PGR)在溃疡型胃癌筛查中的价值。方法 选取行胃镜检查的患者547例,根据胃镜和病理检查结果分为非萎缩性胃炎72例、非萎缩性胃炎伴有其他病理病变232例、萎缩性胃炎42例、消化性溃疡82例、上皮内瘤变15例、胃癌104例(溃疡型胃癌43例,其他型胃癌61例)。采用TRFIA和化学发光微粒子免疫分析法(CMIA)分别检测其中447名胃病患者血浆PGⅠ、PGⅡ水平,并计算PGR值。采用受试者工作特征(ROC)曲线评价PGR诊断溃疡型胃癌的效能。结果 TRFIA与CMIA检测PGⅠ和PGⅡ的结果均呈正相关(r值分别为0.894、0.982,P<0.05)。TRFIA与CMIA检测PGⅠ高值(TRFIA检测PGⅠ的结果≥240 ng/mL)样本的一致性较差。与消化性溃疡组比较,胃癌组血浆PGⅠ水平及PGR显著降低(P<0.05),溃疡型胃癌组PGR显著降低(P<0.05),其他型胃癌组血浆PGⅠ水平显著降低(P<0.05)。溃疡型胃癌组血浆PGⅡ水平及PGR显著高于其他型胃癌组(P<0.05)。PGR诊断溃疡型胃癌的曲线下面积(AUC)为0.711,最佳临界值为18.20,敏感性为72.1%,特异性为70.8%;诊断胃癌的AUC为0.797,最佳临界值为18.37,敏感性为79.8%,特异性为70.8%。结论 TRFIA与CMIA检测PGⅠ、PGⅡ的结果相关性较好,TRFIA检测上限高于CMIA。PGR对溃疡型胃癌有一定的诊断价值。
中图分类号: