
Laboratory Medicine ›› 2025, Vol. 40 ›› Issue (8): 775-781.DOI: 10.3969/j.issn.1673-8640.2025.08.009
Previous Articles Next Articles
GAO Xiantong, YAO Qianqian, RU Lijuan( )
)
Received:2024-03-12
Revised:2024-12-23
Online:2025-08-30
Published:2025-08-28
CLC Number:
GAO Xiantong, YAO Qianqian, RU Lijuan. Establishment and clinical application evaluation of early warning model for acute pancreatitis complicated with AKI[J]. Laboratory Medicine, 2025, 40(8): 775-781.
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.shjyyx.com/EN/10.3969/j.issn.1673-8640.2025.08.009
| 组别 | 例数 | 年龄/岁 | 性别 | 体重指数/(kg·m-2) | 饮酒史/ [例(%)] | 吸烟史/ [例(%)] | 糖尿病史/[例(%)] | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男/[例(%)] | 女/[例(%)] | |||||||||||||||||||
| AKI组 | 41 | 51.00±7.84 | 27(65.85) | 14(34.15) | 24.25±0.52 | 8(19.51) | 24(58.54) | 9(21.95) | ||||||||||||
| 无AKI组 | 59 | 49.52±6.33 | 35(59.32) | 24(40.68) | 24.09±0.64 | 7(11.86) | 28(47.46) | 8(13.56) | ||||||||||||
| 统计值 | 1.042 | 0.438 | 1.325 | 1.110 | 1.190 | 1.207 | ||||||||||||||
| P值 | 0.309 | 0.508 | 0.188 | 0.292 | 0.275 | 0.272 | ||||||||||||||
| 组别 | 冠心病史/ [例(%)] | 高血压史/ [例(%)] | 高脂血症史/[例(%)] | 病因 | 心率/(次·min-1) | |||||||||||||||
| 暴饮暴食/ [例(%)] | 过度饮酒/ [例(%)] | 胆源性/ [例(%)] | ||||||||||||||||||
| AKI组 | 5(12.20) | 7(17.07) | 15(36.59) | 6(14.63) | 10(24.39) | 25(60.98) | 102.25±9.46 | |||||||||||||
| 无AKI组 | 4(6.78) | 12(20.34) | 16(27.12) | 11(18.64) | 15(25.42) | 33(55.93) | 104.00±11.18 | |||||||||||||
| 统计值 | 0.866 | 0.168 | 1.014 | 0.500 | -0.819 | |||||||||||||||
| P值 | 0.352 | 0.682 | 0.314 | 0.617 | 0.415 | |||||||||||||||
| 组别 | 收缩压/Kpa | 舒张压/Kpa | APACHE Ⅱ 评分/分 | SOFA评分/分 | 应用血管活性 药物/[例(%)] | 机械通气/ [例(%)] | 肝功能障碍/[例(%)] | |||||||||||||
| AKI组 | 16.81±0.91 | 11.04±0.72 | 21.59±4.77 | 5.47±0.41 | 17(41.46) | 11(26.83) | 5(12.20) | |||||||||||||
| 无AKI组 | 16.62±1.01 | 10.96±0.84 | 15.00±3.68 | 3.12±0.50 | 9(15.26) | 4(6.78) | 5(8.47) | |||||||||||||
| 统计值 | 0.963 | 0.496 | 7.792 | 24.836 | 8.636 | 7.627 | 0.372 | |||||||||||||
| P值 | 0.338 | 0.621 | <0.001 | <0.001 | 0.003 | 0.006 | 0.542 | |||||||||||||
| 组别 | 例数 | 年龄/岁 | 性别 | 体重指数/(kg·m-2) | 饮酒史/ [例(%)] | 吸烟史/ [例(%)] | 糖尿病史/[例(%)] | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男/[例(%)] | 女/[例(%)] | |||||||||||||||||||
| AKI组 | 41 | 51.00±7.84 | 27(65.85) | 14(34.15) | 24.25±0.52 | 8(19.51) | 24(58.54) | 9(21.95) | ||||||||||||
| 无AKI组 | 59 | 49.52±6.33 | 35(59.32) | 24(40.68) | 24.09±0.64 | 7(11.86) | 28(47.46) | 8(13.56) | ||||||||||||
| 统计值 | 1.042 | 0.438 | 1.325 | 1.110 | 1.190 | 1.207 | ||||||||||||||
| P值 | 0.309 | 0.508 | 0.188 | 0.292 | 0.275 | 0.272 | ||||||||||||||
| 组别 | 冠心病史/ [例(%)] | 高血压史/ [例(%)] | 高脂血症史/[例(%)] | 病因 | 心率/(次·min-1) | |||||||||||||||
| 暴饮暴食/ [例(%)] | 过度饮酒/ [例(%)] | 胆源性/ [例(%)] | ||||||||||||||||||
| AKI组 | 5(12.20) | 7(17.07) | 15(36.59) | 6(14.63) | 10(24.39) | 25(60.98) | 102.25±9.46 | |||||||||||||
| 无AKI组 | 4(6.78) | 12(20.34) | 16(27.12) | 11(18.64) | 15(25.42) | 33(55.93) | 104.00±11.18 | |||||||||||||
| 统计值 | 0.866 | 0.168 | 1.014 | 0.500 | -0.819 | |||||||||||||||
| P值 | 0.352 | 0.682 | 0.314 | 0.617 | 0.415 | |||||||||||||||
| 组别 | 收缩压/Kpa | 舒张压/Kpa | APACHE Ⅱ 评分/分 | SOFA评分/分 | 应用血管活性 药物/[例(%)] | 机械通气/ [例(%)] | 肝功能障碍/[例(%)] | |||||||||||||
| AKI组 | 16.81±0.91 | 11.04±0.72 | 21.59±4.77 | 5.47±0.41 | 17(41.46) | 11(26.83) | 5(12.20) | |||||||||||||
| 无AKI组 | 16.62±1.01 | 10.96±0.84 | 15.00±3.68 | 3.12±0.50 | 9(15.26) | 4(6.78) | 5(8.47) | |||||||||||||
| 统计值 | 0.963 | 0.496 | 7.792 | 24.836 | 8.636 | 7.627 | 0.372 | |||||||||||||
| P值 | 0.338 | 0.621 | <0.001 | <0.001 | 0.003 | 0.006 | 0.542 | |||||||||||||
| 组别 | 例数 | SCr/(μmol·L-1) | L-FABP/(μg·L-1) | KIM-1/(ng·L-1) | Cys C/(μg·L-1) | IL-18/(pg·mL-1) |
|---|---|---|---|---|---|---|
| AKI组 | 41 | 69.00±22.75 | 15.97±5.24 | 50.21±15.75 | 70.88±23.59 | 142.82±42.33 |
| 无AKI组 | 59 | 65.88±11.49 | 10.02±3.31 | 38.66±12.29 | 54.96±18.27 | 109.82±36.14 |
| t值 | 0.902 | 6.958 | 4.114 | 3.799 | 4.185 | |
| P值 | 0.369 | <0.001 | <0.001 | <0.001 | <0.001 |
| 组别 | 例数 | SCr/(μmol·L-1) | L-FABP/(μg·L-1) | KIM-1/(ng·L-1) | Cys C/(μg·L-1) | IL-18/(pg·mL-1) |
|---|---|---|---|---|---|---|
| AKI组 | 41 | 69.00±22.75 | 15.97±5.24 | 50.21±15.75 | 70.88±23.59 | 142.82±42.33 |
| 无AKI组 | 59 | 65.88±11.49 | 10.02±3.31 | 38.66±12.29 | 54.96±18.27 | 109.82±36.14 |
| t值 | 0.902 | 6.958 | 4.114 | 3.799 | 4.185 | |
| P值 | 0.369 | <0.001 | <0.001 | <0.001 | <0.001 |
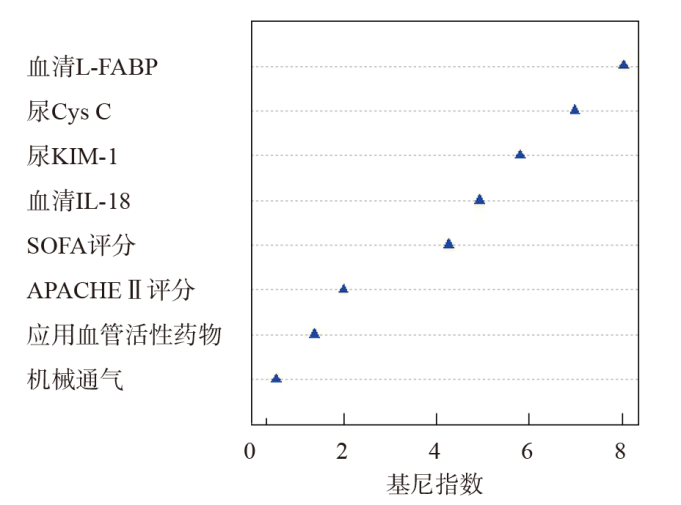
| 项目 | β值 | 标准误 | Wald值 | OR①值(95%CI②) | P值 |
|---|---|---|---|---|---|
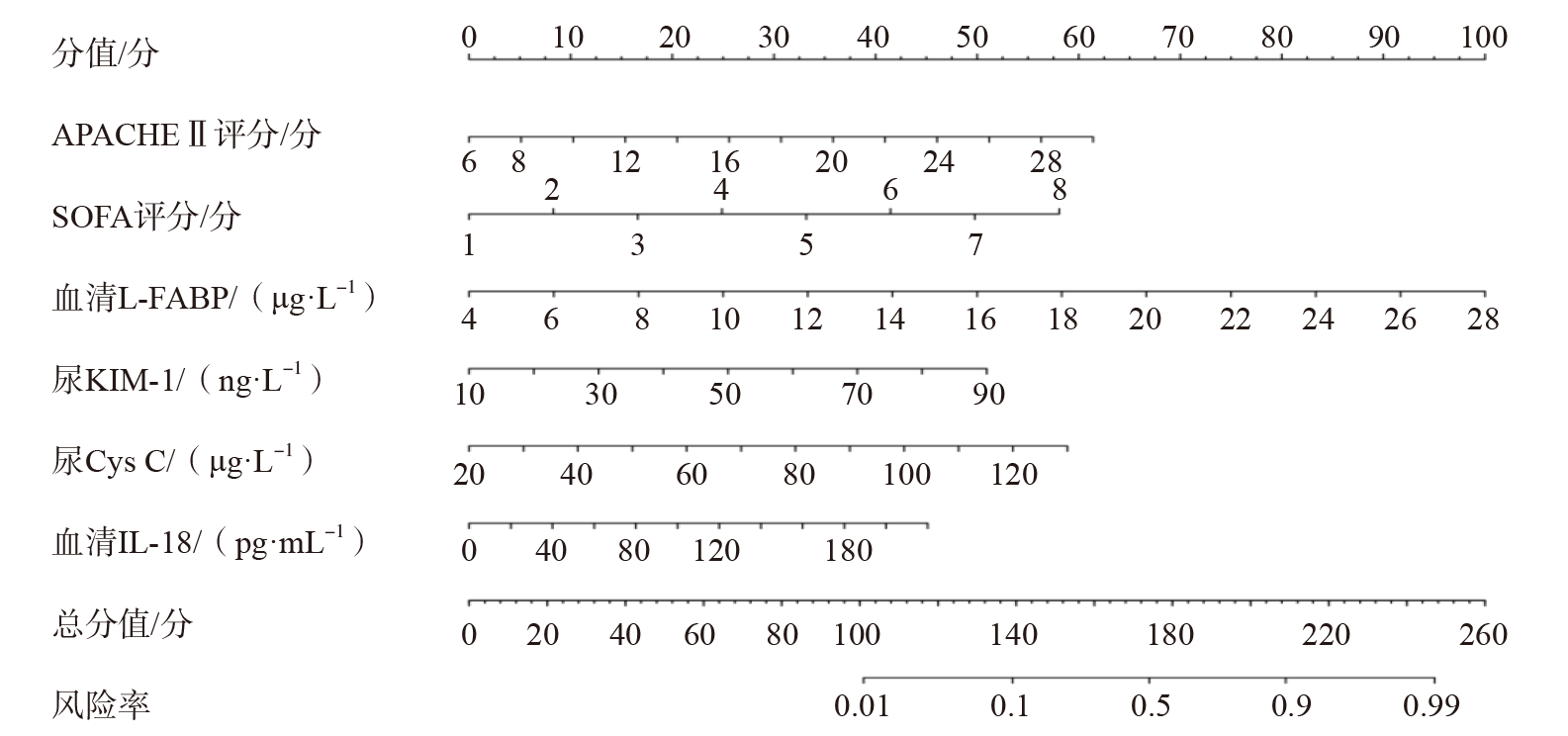
| APACHE Ⅱ评分 | 0.353 | 0.104 | 11.535 | 1.424(1.020~1.987) | <0.001 |
| SOFA评分 | 0.519 | 0.182 | 8.128 | 1.680(1.165~2.423) | 0.006 |
| 血清L-FABP | 0.462 | 0.125 | 13.670 | 1.588(1.436~1.755) | <0.001 |
| 尿KIM-1 | 0.382 | 0.127 | 9.055 | 1.465(1.004~2.139) | <0.001 |
| 尿Cys C | 0.354 | 0.133 | 7.088 | 1.425(1.215~1.671) | 0.019 |
| 血清IL-18 | 0.225 | 0.096 | 5.480 | 1.252(1.118~1.402) | 0.035 |
| 项目 | β值 | 标准误 | Wald值 | OR①值(95%CI②) | P值 |
|---|---|---|---|---|---|
| APACHE Ⅱ评分 | 0.353 | 0.104 | 11.535 | 1.424(1.020~1.987) | <0.001 |
| SOFA评分 | 0.519 | 0.182 | 8.128 | 1.680(1.165~2.423) | 0.006 |
| 血清L-FABP | 0.462 | 0.125 | 13.670 | 1.588(1.436~1.755) | <0.001 |
| 尿KIM-1 | 0.382 | 0.127 | 9.055 | 1.465(1.004~2.139) | <0.001 |
| 尿Cys C | 0.354 | 0.133 | 7.088 | 1.425(1.215~1.671) | 0.019 |
| 血清IL-18 | 0.225 | 0.096 | 5.480 | 1.252(1.118~1.402) | 0.035 |

注: 全部; 无; 模型。
| [1] | SZATMARY P, GRAMMATIKOPOULOS T, CAI W, et al. Acute pancreatitis:diagnosis and treatment[J]. Drugs, 2022, 82(12):1251-1276. |
| [2] | PATEL D B, FARRIS A C, HANNA C, et al. Concurrent acute kidney injury and pancreatitis in a female patient:answers[J]. Pediatr Nephrol, 2023, 38(4):1047-1050. |
| [3] | WU S, ZHOU Q, CAI Y, et al. Development and validation of a prediction model for the early occurrence of acute kidney injury in patients with acute pancreatitis[J]. Ren Fail, 2023, 45(1):2194436. |
| [4] | PORSCHEN C, STRAUSS C, MEERSCH M, et al. Personalized acute kidney injury treatment[J]. Curr Opin Crit Care, 2023, 29(6):551-558. |
| [5] | DAI X Y, HU Q, YAO J Q, et al. Zengye decoction attenuated severe acute pancreatitis complicated with acute kidney injury by modulating the gut microbiome and serum amino acid metabolome[J]. Evid Based Complement Alternat Med, 2022,2022:1588786. |
| [6] | YANG Y, XIAO W, LIU X, et al. Machine learning-assisted ensemble analysis for the prediction of acute pancreatitis with acute kidney injury[J]. Int J Gen Med, 2022,15:5061-5072. |
| [7] | 中华医学会消化病学分会胰腺疾病学组,《中华胰腺病杂志》编委会,《中华消化杂志》编委会. 中国急性胰腺炎诊治指南(2019年,沈阳)[J]. 临床肝胆病杂志, 2019, 35(12):2706-2711. |
| [8] | KELLUM J A, LAMEIRE N, KDIGO AKI Guideline Work Group. Diagnosis,evaluation,and management of acute kidney injury:a KDIGO summary(Part 1)[J]. Crit Care, 2013, 17(1):204. |
| [9] | CHENG Y, YANG J, WU Q, et al. Machine learning for the prediction of acute kidney injury in patients with acute pancreatitis admitted to the intensive care unit[J]. Chin Med J(Engl), 2022, 135(23):2886-2887. |
| [10] | SHI N, SUN G D, JI Y Y, et al. Effects of acute kidney injury on acute pancreatitis patients' survival rate in intensive care unit:a retrospective study[J]. World J Gastroenterol, 2021, 27(38):6453-6464. |
| [11] | SELVANATHAN D K, JOHNSON P G, THANIKACHALAM D K, et al. Acute kidney injury complicating severe acute pancreatitis:clinical profile and factors predicting mortality[J]. Indian J Nephrol, 2022, 32(5):460-466. |
| [12] | ZHAO X, LU Y, LI S, et al. Predicting renal function recovery and short-term reversibility among acute kidney injury patients in the ICU:comparison of machine learning methods and conventional regression[J]. Ren Fail, 2022, 44(1):1326-1337. |
| [13] | 李晓玲, 李芳芳, 尹佳萌, 等. 血清中性粒细胞明胶酶相关载脂蛋白、核转录因子-κB及血清肌酐对重症急性胰腺炎伴急性肾损伤的预测价值[J]. 中华生物医学工程杂志, 2022, 28(1):49-53. |
| [14] | OKUDA H, OBATA Y, KAMIJO-IKEMORI A, et al. Quantitative and qualitative analyses of urinary L-FABP for predicting acute kidney injury after emergency laparotomy[J]. J Anesth, 2022, 36(1):38-45. |
| [15] | WEN Y, PARIKH C R. Current concepts and advances in biomarkers of acute kidney injury[J]. Crit Rev Clin Lab Sci, 2021, 58(5):354-368. |
| [16] | BRIGUORI C, QUINTAVALLE C, DONNARUMMA E, et al. Novel biomarkers for contrast-induced acute kidney injury[J]. Biomed Res Int, 2014,2014:568738. |
| [17] | 柯贵宝, 刘哲, 徐云滢, 等. L-FABP和NAG在重症急性胰腺炎合并急性肾损伤中的早期诊断价值[J]. 现代临床医学, 2015(4):263-264. |
| [18] | CAFAROTTI A, MARCOVECCHIO M L, LAPERGOLA G, et al. Kidney function and renal resistive index in children with juvenile idiopathic arthritis[J]. Clin Exp Med, 2023, 23(3):759-766. |
| [19] | JIANG R, HUANG Y, ZENG M, et al. A marked elevation in serum creatinine/cystatin C ratio may indicate pseudo-acute kidney injury due to urinary ascites:a case report and literature review[J]. BMC Nephrol, 2023, 24(1):243. |
| [20] |
延喜胜, 雷磊, 王剑. 幽门螺杆菌毒力基因分型与消化性溃疡患者早期肾损伤相关性研究[J]. 检验医学, 2022, 37(1):16-22.
DOI |
| [21] |
朱庆华, 王伟伟, 邹广慧, 等. 血清NGAL和Cys C联合检测在诊断2型糖尿病早期肾损伤中的价值[J]. 检验医学, 2021, 36(3):281-284.
DOI |
| [22] | BRILLAND B, BOUD'HORS C, WACRENIER S, et al. Kidney injury molecule 1(KIM-1):a potential biomarker of acute kidney injury and tubulointerstitial injury in patients with ANCA-glomerulonephritis[J]. Clin Kidney J, 2023, 16(9):1521-1533. |
| [23] | 李振翮, 王贵霞, 甄国栋, 等. 血清SIRT1和Syndecan-1水平变化对重症急性胰腺炎合并急性肾损伤患者病情和临床转归的预测研究[J]. 临床急诊杂志, 2024, 25(1):32-37. |
| [24] | LIU Y H, CHEN Y H, KO C H, et al. SOD3 and IL-18 predict the first kidney disease-related hospitalization or death during the one-year follow-up period in patients with end-stage renal disease[J]. Antioxidants(Basel), 2022, 11(6):1198. |
| [25] | 宋微, 李虹怡, 吕洪波. 血清miR-21-3p、IL-18水平对重症急性胰腺炎患者急性肾损伤的预测价值[J]. 山东医药, 2022, 62(1):20-24. |
| [26] | TEJCHMAN K, NOWACKI A, KOTFIS K, et al. The role of endothelins,IL-18,and NGAL in kidney hypothermic machine perfusion[J]. Biomedicines, 2021, 9(4):417. |
| [27] | 廖小胖, 邹晓东, 于博, 等. 甘油三酯-葡萄糖指数与中度重症及重症急性胰腺炎并发急性肾损伤的相关性[J]. 实用临床医药杂志, 2023, 27(9):106-110. |
| [1] | KE Wencai, LIU Jie, LIN Yong, LU Guangjian, JIAO Luyang. Establishment and verification of nomogram diagnostic model of osteoporosis in elders based on laboratory indicators [J]. Laboratory Medicine, 2025, 40(8): 735-741. |
| [2] | Yueyang Hospital of Integrated Traditional Chinese and Western Medicine of Shanghai University of Traditional Chinese Medicine Shanghai Center for Clinical Laboratory, Clinical Laboratory Society of Chinese Association for Rehabilitation Medicine Clinical Laboratory Society of Chinese Association of Integrative Medicine, Tumor Immunology Branch of Shanghai Society for Immunology Molecular Diagnostics Society of Shanghai Medical Association. Expert consensus on non-invasive laboratory diagnosis for hepatic fibrosis [J]. Laboratory Medicine, 2025, 40(7): 625-641. |
| [3] | GUO Fengxia, HU Bing, SHA Yanhua. Role of methyltransferase-like protein 14 in patients with coronary heart disease [J]. Laboratory Medicine, 2025, 40(1): 54-58. |
| [4] | ZOU Chen, XU Runhao, DING Yi, ZHANG Jie, WENG Wenhao, WANG Zhenhua, CAO Yun. Colorectal cancer screening model based on ProteomeXchange database [J]. Laboratory Medicine, 2024, 39(12): 1181-1189. |
| [5] | LEI Ming, ZHAI Li, WEI Ying, LIN Yichen, GUO Mengyue. Application of nomogram model based on clinical characteristics and serum tumor markers in differential diagnosis of benign and malignant lung lesions [J]. Laboratory Medicine, 2024, 39(10): 956-962. |
| [6] | SUN Zepeng, WANG Hongbin, WANG Jiandong, SONG Dewei, XIAO Peng. Analysis and progress of peptide and protein biomarker methodology for myocardial injury [J]. Laboratory Medicine, 2023, 38(8): 784-789. |
| [7] | WANG Haiping, LI He. BISAP score combined with serum sRAGE for predicting hyperlipidemic acute pancreatitis severity and short-term prognosis [J]. Laboratory Medicine, 2023, 38(7): 653-658. |
| [8] | ZHANG Min, WANG Binyu, CHI Weiqun, LIU Yu. Research progress of exosomal non-coding RNA as biomarkers for disease diagnosis [J]. Laboratory Medicine, 2023, 38(6): 594-598. |
| [9] | GAO Feng. Clinical application of novel tumor biomarkers:prospects and challenges [J]. Laboratory Medicine, 2023, 38(4): 303-306. |
| [10] | ZHOU Furong, LI Yanzhu, LIU Yonggan. Application of lncRNA SNP in colorectal cancer susceptibility prediction and prognosis assessment [J]. Laboratory Medicine, 2023, 38(12): 1206-1210. |
| [11] | LU Qiyuan, LU Jianhua. Biomarker research progress for the diagnosis of periprosthetic joint infection [J]. Laboratory Medicine, 2023, 38(10): 997-1002. |
| [12] | CHEN Xuewei, LI Yirong. Candidate biomarkers in metabolic syndrome based on GEO database [J]. Laboratory Medicine, 2023, 38(1): 32-38. |
| [13] | WU Yating, LI Zhuolin, LEI Yan, JIA Ruxue, ZHANG Shenghang, WANG Shuiliang. Research progress of miRNA in urine as a biomarker for common malignant tumors [J]. Laboratory Medicine, 2023, 38(1): 94-99. |
| [14] | WANG Rui, LI Zhaoyan, ZHAO Aiguang. Application of circulating tumor DNA detection in the diagnosis and treatment of gastric cancer [J]. Laboratory Medicine, 2022, 37(9): 877-881. |
| [15] | WU Yanqian, YU Chong, SHEN Lu, ZHENG Haoran, HONG Yeting. Research progress of body fluid piRNA as a potential biomarker of disease [J]. Laboratory Medicine, 2022, 37(8): 782-786. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||