检验医学 ›› 2024, Vol. 39 ›› Issue (11): 1072-1077.DOI: 10.3969/j.issn.1673-8640.2024.11.008
胡传玺, 刘灵燕, 李漫( )
)
HU Chuanxi, LIU Lingyan, LI Man()
摘要:
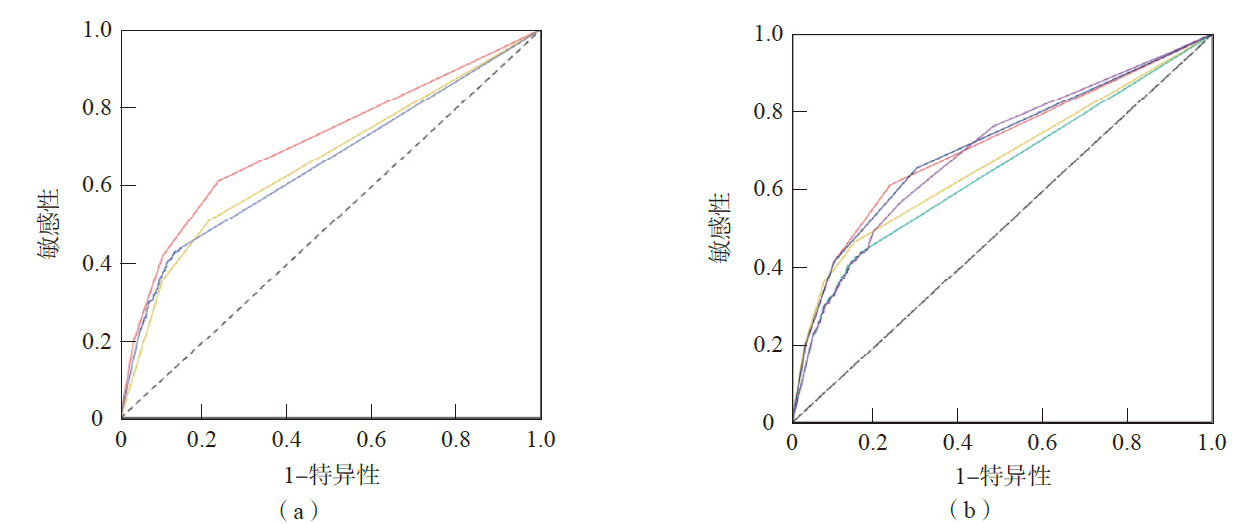
目的 探讨间接免疫荧光法(IFA)、线性免疫印迹法(LIA)、化学发光法(CLIA)单独和联合检测抗核抗体(ANA)的临床价值。方法 选取2022年8月—2023年7月在上海交通大学医学院附属第九人民医院进行ANA检测的患者4 722例,其中自身免疫性疾病(AID)患者935例(AID组)、非AID患者3 787例(非AID组)。采用IFA检测ANA,采用LIA、CLIA 检测特异性ANA谱。采用Kappa一致性检验评估不同方法之间的一致性。采用受试者工作特征(ROC)曲线评价不同方法诊断AID的效能。结果 AID组IFA、LIA、CLIA阳性检出率分别为67.5%、52.1%、44.8%,均高于非AID组(36.9%、20.1%、17.4%)(P<0.05)。IFA与LIA的一致性一般(Kappa=0.609),IFA与CLIA的一致性差(Kappa=0.276)。在不同类型疾病患者中,AID患者的一致性最高(IFA与LIA、CLIA的kappa值分别为0.628、0.444),其他疾病类型患者的一致程度最低(IFA与LIA、CLIA的kappa值分别为0.120、0.194)。IFA、LIA、CLIA单项检测诊断AID的曲线下面积(AUC)分别为0.707、0.662、0.655。IFA和LIA并联、IFA和CLIA并联检测诊断AID的AUC分别为0.711、0.699,IFA和LIA串联、IFA和CLIA串联检测诊断AID的AUC分别为0.677、0.647。结论 IFA与LIA、CLIA的一致性不高,且检测结果不一致的情况更可能出现在非AID患者中。使用单项检测方法进行AID筛查时,应优先采用IFA检测ANA;若采用ANA和特异性ANA谱联合检测,以并联方式为宜。
中图分类号: