
Laboratory Medicine ›› 2023, Vol. 38 ›› Issue (6): 532-537.DOI: 10.3969/j.issn.1673-8640.2023.06.005
Previous Articles Next Articles
LIU Yanan, XIA Min, HU Shaohua, ZHENG Yue, ZHANG Hong( )
)
Received:2022-07-13
Revised:2023-03-10
Online:2023-06-30
Published:2023-08-22
CLC Number:
LIU Yanan, XIA Min, HU Shaohua, ZHENG Yue, ZHANG Hong. Roles of lymphocyte subsets,inflammatory factors and NT-proBNP in diagnosis of Kawasaki disease[J]. Laboratory Medicine, 2023, 38(6): 532-537.
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.shjyyx.com/EN/10.3969/j.issn.1673-8640.2023.06.005
| 组别 | 例数 | IL-8 | IL-1β | IL-2 | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | |||||||||
| KD组 | 222 | 0.10 | 20.40 | 323.56 | 574.34 | 0.10 | 0.10 | 2.74 | 6.88 | 0.10 | 0.10 | 0.10 | 2.75 | |||||||
| 感染发热组 | 177 | 0.10 | 0.10 | 18.08 | 101.09 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | |||||||
| Z值 | -5.347 | -3.812 | -1.893 | |||||||||||||||||
| P值 | <0.001 | <0.001 | 0.058 | |||||||||||||||||
| 组别 | IL-6 | IL-10 | IL-4 | IL-5 | ||||||||||||||||
| P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | |||||
| KD组 | 0.10 | 25.11 | 14.91 | 357.13 | 0.10 | 7.64 | 29.48 | 60.92 | 0.10 | 0.10 | 0.10 | 5.89 | 0.10 | 0.10 | 0.10 | 5.89 | ||||
| 感染发热组 | 0.10 | 0.10 | 0.10 | 0.29 | 0.10 | 0.10 | 3.02 | 15.41 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | ||||
| Z值 | -7.314 | -6.687 | -3.008 | -3.239 | ||||||||||||||||
| P值 | <0.001 | <0.001 | <0.001 | 0.001 | ||||||||||||||||
| 组别 | IL-12P70 | IL-17A | IL-18 | |||||||||||||||||
| P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | |||||||||
| 感染发热组 | 0.10 | 0.10 | 0.10 | 22.85 | 0.10 | 0.10 | 0.10 | 0.60 | 0.10 | 7.95 | 136.64 | 191.66 | ||||||||
| KD组 | 0.10 | 0.10 | 0.10 | 27.85 | 0.10 | 0.10 | 0.91 | 1.70 | 18.90 | 75.51 | 148.66 | 252.16 | ||||||||
| Z值 | -2.856 | -4.178 | -5.950 | |||||||||||||||||
| P值 | 0.004 | <0.001 | <0.001 | |||||||||||||||||
| 组别 | TNF-α | INF-γ | sCD25 | |||||||||||||||||
| P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | |||||||||
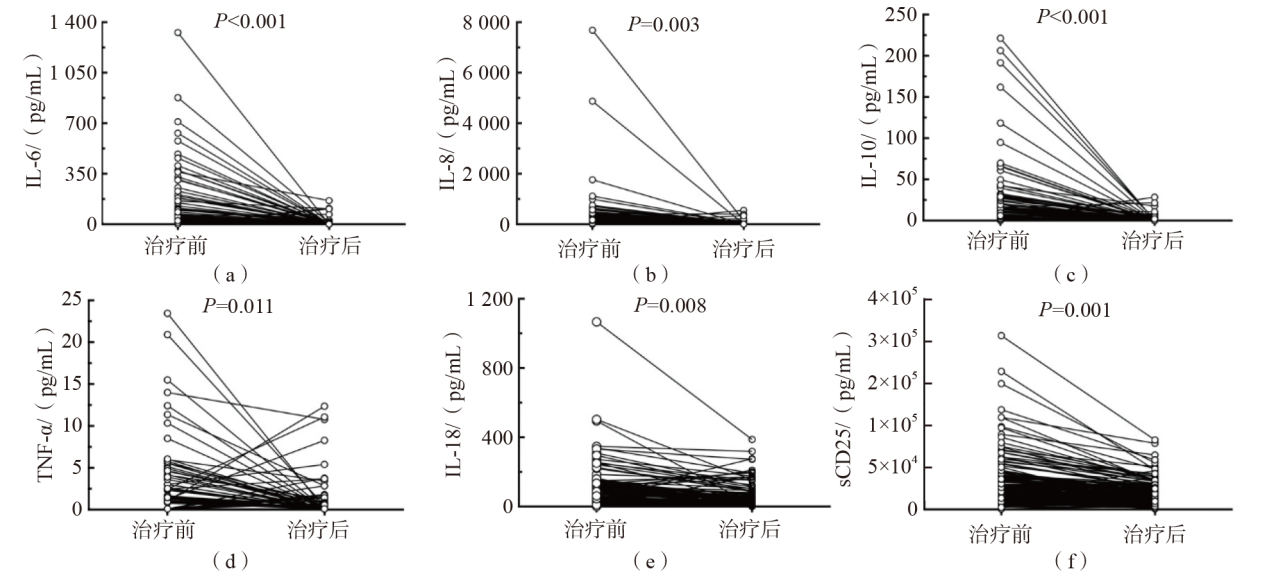
| KD组 | 0.10 | 0.10 | 3.01 | 5.75 | 0.23 | 2.77 | 20.06 | 112.48 | 27 214.81 | 47 688.36 | 92 148.49 | 126 074.00 | ||||||||
| 感染发热组 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 1.00 | 26.21 | 47.45 | 15 896.00 | 23 829.98 | 32 245.89 | 36 403.40 | ||||||||
| Z值 | -5.420 | -3.628 | -7.521 | |||||||||||||||||
| P值 | <0.001 | <0.001 | <0.001 | |||||||||||||||||
| 组别 | 例数 | IL-8 | IL-1β | IL-2 | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | |||||||||
| KD组 | 222 | 0.10 | 20.40 | 323.56 | 574.34 | 0.10 | 0.10 | 2.74 | 6.88 | 0.10 | 0.10 | 0.10 | 2.75 | |||||||
| 感染发热组 | 177 | 0.10 | 0.10 | 18.08 | 101.09 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | |||||||
| Z值 | -5.347 | -3.812 | -1.893 | |||||||||||||||||
| P值 | <0.001 | <0.001 | 0.058 | |||||||||||||||||
| 组别 | IL-6 | IL-10 | IL-4 | IL-5 | ||||||||||||||||
| P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | |||||
| KD组 | 0.10 | 25.11 | 14.91 | 357.13 | 0.10 | 7.64 | 29.48 | 60.92 | 0.10 | 0.10 | 0.10 | 5.89 | 0.10 | 0.10 | 0.10 | 5.89 | ||||
| 感染发热组 | 0.10 | 0.10 | 0.10 | 0.29 | 0.10 | 0.10 | 3.02 | 15.41 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | ||||
| Z值 | -7.314 | -6.687 | -3.008 | -3.239 | ||||||||||||||||
| P值 | <0.001 | <0.001 | <0.001 | 0.001 | ||||||||||||||||
| 组别 | IL-12P70 | IL-17A | IL-18 | |||||||||||||||||
| P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | |||||||||
| 感染发热组 | 0.10 | 0.10 | 0.10 | 22.85 | 0.10 | 0.10 | 0.10 | 0.60 | 0.10 | 7.95 | 136.64 | 191.66 | ||||||||
| KD组 | 0.10 | 0.10 | 0.10 | 27.85 | 0.10 | 0.10 | 0.91 | 1.70 | 18.90 | 75.51 | 148.66 | 252.16 | ||||||||
| Z值 | -2.856 | -4.178 | -5.950 | |||||||||||||||||
| P值 | 0.004 | <0.001 | <0.001 | |||||||||||||||||
| 组别 | TNF-α | INF-γ | sCD25 | |||||||||||||||||
| P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | P50 | P75 | P90 | P95 | |||||||||
| KD组 | 0.10 | 0.10 | 3.01 | 5.75 | 0.23 | 2.77 | 20.06 | 112.48 | 27 214.81 | 47 688.36 | 92 148.49 | 126 074.00 | ||||||||
| 感染发热组 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 1.00 | 26.21 | 47.45 | 15 896.00 | 23 829.98 | 32 245.89 | 36 403.40 | ||||||||
| Z值 | -5.420 | -3.628 | -7.521 | |||||||||||||||||
| P值 | <0.001 | <0.001 | <0.001 | |||||||||||||||||
| 统计值 | IL-8 | IL-1β | IL-2 | IL-6 | IL-10 | IL-4 | IL-5 | IL-12P70 | IL-17A | IL-18 | TNF-α | INF-γ | sCD25 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r值 | -0.028 | 0.100 | -0.153 | 0.416 | 0.407 | -0.047 | 0.100 | 0.116 | 0.259 | 0.256 | 0.308 | 0.238 | 0.531 | |
| P值 | 0.738 | 0.231 | 0.066 | <0.001 | <0.001 | 0.574 | 0.230 | 0.164 | 0.002 | 0.002 | <0.001 | 0.004 | <0.001 | |
| 统计值 | IL-8 | IL-1β | IL-2 | IL-6 | IL-10 | IL-4 | IL-5 | IL-12P70 | IL-17A | IL-18 | TNF-α | INF-γ | sCD25 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r值 | -0.028 | 0.100 | -0.153 | 0.416 | 0.407 | -0.047 | 0.100 | 0.116 | 0.259 | 0.256 | 0.308 | 0.238 | 0.531 | |
| P值 | 0.738 | 0.231 | 0.066 | <0.001 | <0.001 | 0.574 | 0.230 | 0.164 | 0.002 | 0.002 | <0.001 | 0.004 | <0.001 | |
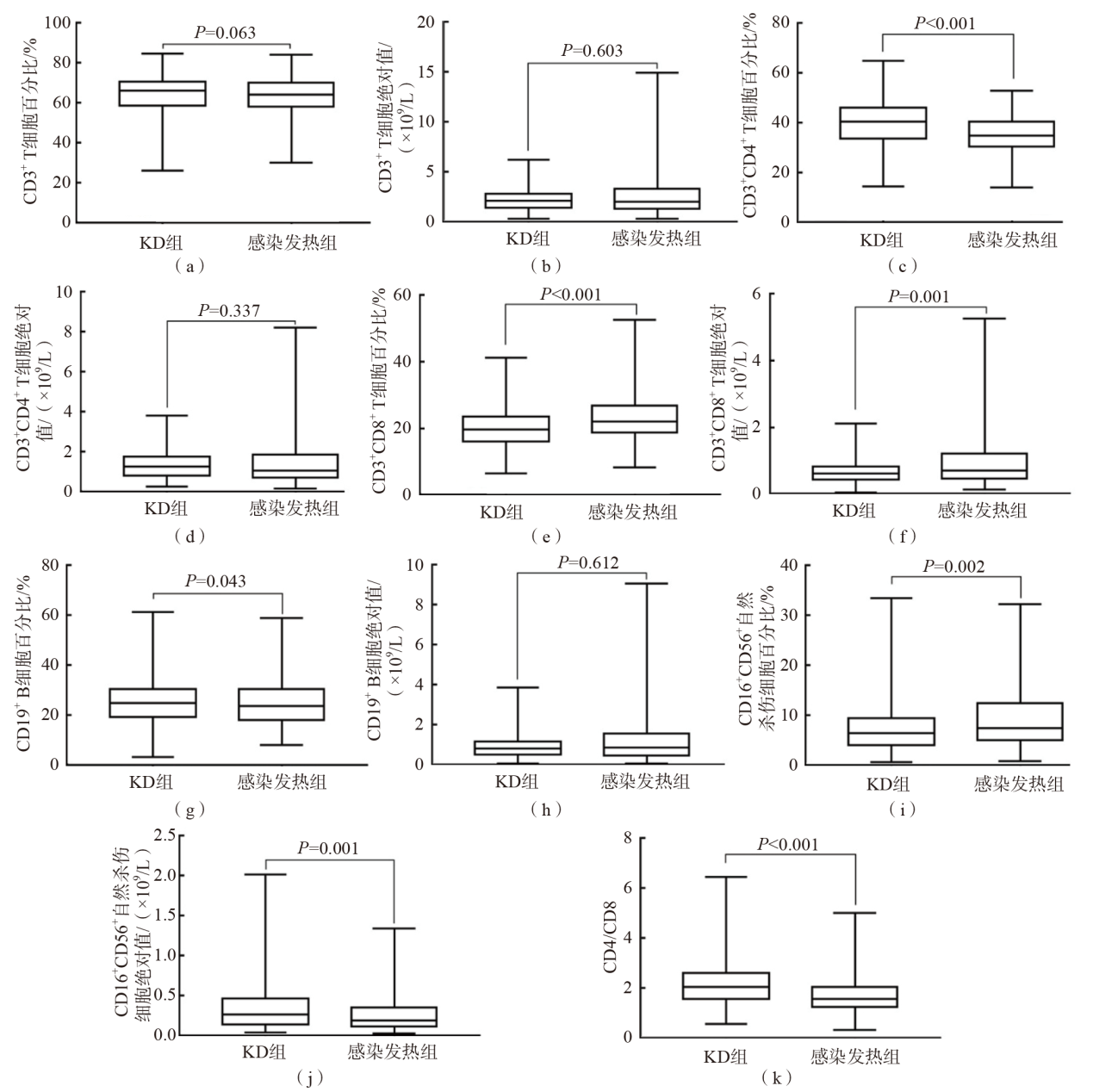
| 统计值 | CD3+ T细胞 | CD3+CD8+ T细胞 | CD16+CD56+自然杀伤细胞 | CD19+ B细胞 | CD4/CD8比值 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 百分比 | 绝对值 | 百分比 | 绝对值 | 百分比 | 绝对值 | 百分比 | 绝对值 | |||||
| r值 | -0.116 | 0.075 | -0.241 | -0.032 | -0.147 | -0.088 | 0.218 | 0.190 | 0.197 | |||
| P值 | 0.165 | 0.368 | 0.003 | 0.702 | 0.077 | 0.291 | 0.008 | 0.022 | 0.017 | |||
| 统计值 | CD3+ T细胞 | CD3+CD8+ T细胞 | CD16+CD56+自然杀伤细胞 | CD19+ B细胞 | CD4/CD8比值 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 百分比 | 绝对值 | 百分比 | 绝对值 | 百分比 | 绝对值 | 百分比 | 绝对值 | |||||
| r值 | -0.116 | 0.075 | -0.241 | -0.032 | -0.147 | -0.088 | 0.218 | 0.190 | 0.197 | |||
| P值 | 0.165 | 0.368 | 0.003 | 0.702 | 0.077 | 0.291 | 0.008 | 0.022 | 0.017 | |||
| [1] |
ROWLEY A H, SHULMAN S T. The epidemiology and pathogenesis of Kawasaki disease[J]. Front Pediatr, 2018, 6:374.
DOI PMID |
| [2] |
RIFE E, GEDALIA A. Kawasaki disease:an update[J]. Curr Rheumatol Rep, 2020, 22(10):75.
DOI |
| [3] |
JCS Joint Working Group. Guidelines for diagnosis and management of cardiovascular sequelae in Kawasaki disease(JCS 2013). Digest version[J]. Circ J, 2014, 78(10):2521-2562.
DOI URL |
| [4] |
NAGATA S. Causes of Kawasaki disease-from past to present[J]. Front Pediatr, 2019, 7:18.
DOI PMID |
| [5] |
DEL PRINCIPE D, PIETRAFORTE D, GAMBARDELLA L, et al. Pathogenetic determinants in Kawasaki disease:the haematological point of view[J]. J Cell Mol Med, 2017, 21(4):632-639.
DOI URL |
| [6] |
SWANSON K V, DENG M, TING J P. The NLRP3 inflammasome:molecular activation and regulation to therapeutics[J]. Nat Rev Immunol, 2019, 19(8):477-489.
DOI |
| [7] |
KIM K Y, KIM D S. Recent advances in Kawasaki disease[J]. Yonsei Med J, 2016, 57(1):15-21.
DOI PMID |
| [8] |
WENG K P, HSIEH K S, HUANG S H, et al. Interleukin-18 and coronary artery lesions in patients with Kawasaki disease[J]. J Chin Med Assoc, 2013, 76(8):438-445.
DOI URL |
| [9] |
TERAURA H, KOTANI K, MINAMI T, et al. The serum concentration of soluble interleukin-2 receptor in patients with Kawasaki disease[J]. Ann Clin Biochem, 2017, 54(2):209-213.
DOI PMID |
| [10] |
WU L, CHEN Y, ZHONG S, et al. Blood N-terminal pro-brain natriuretic peptide and interleukin-17 for distinguishing incomplete Kawasaki disease from infectious diseases[J]. Indian Pediatr, 2015, 52(6):477-480.
PMID |
| [11] | 丁艳, 尹薇, 王瑞耕, 等. 川崎病患儿淋巴细胞亚群及免疫球蛋白的变化[J]. 临床儿科杂志, 2016, 34(1):29-32. |
| [12] | 汪希珂, 刘晓英, 吴悦, 等. T细胞免疫及细胞因子在川崎病不同时期表达变化的研究[J]. 贵州医药, 2018, 42(3):276-280. |
| [13] | 祝绚, 王雪梅, 刘成桂, 等. 川崎病患儿外周血淋巴细胞亚群变化及临床意义[J]. 国际检验医学杂志, 2016, 37(10):1393-1395. |
| [14] |
LINDQUIST M E, HICAR M D. B cells and antibodies in Kawasaki disease[J]. Int J Mol Sci, 2019, 20(8):1834.
DOI URL |
| [15] |
ZHENG X, ZHANG Y, LIU L, et al. N-terminal pro-brain natriuretic peptide as a biomarker for predicting coronary artery lesion of Kawasaki disease[J]. Sci Rep, 2020, 10(1):5130.
DOI PMID |
| [16] | DIONNE A, DAHDAH N. A decade of NT-proBNP in acute Kawasaki disease,from physiological response to clinical relevance[J]. Children(Basel), 2018, 5(10):141. |
| [17] |
YANAGISAWA D, AYUSAWA M, KATO M, et al. Factors affecting N-terminal pro-brain natriuretic peptide elevation in the acute phase of Kawasaki disease[J]. Pediatr Int, 2016, 58(11):1105-1111.
DOI PMID |
| [1] | ZHAI Bin, HAN Mei. Expression changes of serum miR-21 and miR-146a in children with Mycoplasma pneumoniae pneumonia and their correlation with inflammatory factors [J]. Laboratory Medicine, 2024, 39(8): 787-792. |
| [2] | ZHENG Hui, CHEN Yingxiu, YE Lüyin, LU Renquan, GUO Lin. Relationship between peripheral blood T lymphocyte subsets and tumor progression in patients with colorectal cancer [J]. Laboratory Medicine, 2024, 39(4): 330-335. |
| [3] | LIANG Zhenlong, GUO Yuni, WANG Nan, WANG Jianan, LIU Jiayu, LIU Peipei, XIANG Daijun, WANG Chengbin, LI Mianyang. Clinical role of lymphocyte subsets in graft-versus-host disease patients after hematopoietic stem cell transplantation [J]. Laboratory Medicine, 2024, 39(4): 387-392. |
| [4] | JING Lanting, ZHU Mengting, YANG Zhenkun, LUO Yuanyuan, ZOU Jian, YIN Ying. Application of CD14 reverse assisted gate method in detection of lymphocyte subsets [J]. Laboratory Medicine, 2024, 39(3): 227-236. |
| [5] | PENG Wei, LI Yungai, XU Jing, LIU Hua, YANG Cuixia, SHEN Yunyue. Serum inflammatory factors combined with PSA and f-PSA in the auxiliary diagnosis of prostate cancer [J]. Laboratory Medicine, 2023, 38(9): 849-854. |
| [6] | YIN Ya, PAN Yuan, ZHOU Hongwei, SHEN Wei. Application progress of BNP and NT-proBNP in neonates [J]. Laboratory Medicine, 2023, 38(6): 518-523. |
| [7] | LI Li, SUN Haiyan, LI Yuanrui, DOU Min, TANG Wen, JIANG Limin, SHEN Lisong. Changes and clinical roles of perioperative NT-proBNP and PCT in children with congenital heart disease [J]. Laboratory Medicine, 2023, 38(6): 524-531. |
| [8] | TAN Meiyu, SHU Jie, XUAN Binbin, ZHOU Lida, LI Hong, HOU Shangwei, SHENG Huiming. Effects of SARS-CoV-2 vaccination on antibody production and immune function [J]. Laboratory Medicine, 2022, 37(8): 729-734. |
| [9] | JU Yinghui, MO Huifang, WU Hui, CHEN Pu, GUO Wei, WANG Beili. Performance comparison of lymphocyte subset determination by 6-color flow cytometry with 2 different reagents [J]. Laboratory Medicine, 2022, 37(3): 270-273. |
| [10] | XUE Yan, XU Li, DANG Liheng, WANG Chao, CUI Yaqiong, WANG Ping, WANG Ning, ZHANG Xinjie, LIU Yang. Interference of high levels of bilirubin on lymphocyte subset determination in peripheral blood by flow cytometry and its elimination methods [J]. Laboratory Medicine, 2022, 37(12): 1169-1173. |
| [11] | ZHAO Qian, HU Hongxia. Roles of serum ACTA,LXA4,Tau protein in prognostic evaluation of children with hypoxic-ischemic encephalopathy [J]. Laboratory Medicine, 2022, 37(11): 1057-1061. |
| [12] | WANG Zhifeng, ZHOU Yang, DING Yina, DANG Jianhong, HU Dian, JIN Zhijun. Roles of peripheral blood inflammatory factors and coagulation indicators in endometriosis patients with pelvic adhesion [J]. Laboratory Medicine, 2021, 36(10): 1050-1054. |
| [13] | CHEN Bin, LU Weiwei, XU Zhongyu. Roles of serum NT-proBNP,CRP and MMP-9 in children with Kawasaki disease [J]. Laboratory Medicine, 2020, 35(3): 243-246. |
| [14] | LIU Yunfeng, ZHENG Hao, CHE Di, PI Lei, FU Lanyan, GU Xiaoqiong. Role of berberine on anti-platelet aggregation in children with Kawasaki disease in vitro [J]. Laboratory Medicine, 2020, 35(11): 1158-1160. |
| [15] | CHEN Shiyang, FU Xiaoying, XU Gang, LIN Zhenhu, LUO Meizhu, MAI Huirong, CHEN Yunsheng, LIU Sixi. Monitoring lymphocyte subsets after β-mediterranean anemia allogeneic hematopoetic stem cell transplantation in children [J]. Laboratory Medicine, 2019, 34(12): 1066-1071. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||