
检验医学 ›› 2023, Vol. 38 ›› Issue (7): 653-658.DOI: 10.3969/j.issn.1673-8640.2023.07.007
汪海平, 李贺( )
)
收稿日期:2022-12-01
修回日期:2023-01-15
出版日期:2023-07-30
发布日期:2023-09-18
通讯作者:
李 贺,E-mail:422600897@qq.com。
作者简介:汪海平,男,1985年生,硕士,主治医师,主要从事急腹症和创伤类疾病的诊治工作。
WANG Haiping, LI He()
Received:2022-12-01
Revised:2023-01-15
Online:2023-07-30
Published:2023-09-18
摘要:
目的 探讨急性胰腺炎严重程度床旁指数(BISAP)评分联合血清可溶性晚期糖基化终产物受体(sRAGE)对急性高脂血症性胰腺炎(HLAP)严重程度和预后评估的价值。方法 选取2017年3月—2022年8月安徽医科大学第二附属医院HLAP患者142例。对所有患者行急性生理与慢性健康评分Ⅱ(APACHE Ⅱ)、序贯器官衰竭估计(SOFA)评分和BISAP评分。收集所有患者的临床资料和实验室检测结果,并检测血清sRAGE水平。根据BISAP评分结果将患者分为重症HLAP(重症组,54例)和非重症HLAP(非重症组,88例)。根据患者入院30 d的生存状态分为死亡组(42例)和非死亡组(100例)。采用Logistic回归分析评估HLAP患者入院30 d死亡的危险因素。采用受试者工作特征(ROC)曲线评价各项指标鉴别诊断重症HLAP和判断HLAP患者入院30 d死亡的效能。结果 与非重症组比较,重症组APACHE Ⅱ评分、SOFA评分和sRAGE水平均显著升高(P<0.05)。与非死亡组比较,死亡组C反应蛋白(CRP)、sRAGE水平和BISAP评分≥3分所占比例、APACHE Ⅱ评分、SOFA评分均显著升高(P<0.05)。多因素Logistic回归分析结果显示,APACHE Ⅱ评分升高和sRAGE水平升高均是重症HLAP的危险因素[比值比(OR)值分别为1.17和1.01,95%可信区间(CI)分别为1.03~1.34和1.00~1.01]。BISAP评分≥3分和血清sRAGE水平是HLAP患者入院30 d死亡的危险因素(OR值分别为1.99和1.01,95%CI分别为1.53~2.98和1.00~1.03)。sRAGE鉴别诊断重症HLAP的曲线下面积(AUC)为0.73。BISAP评分、sRAGE单项和联合检测判断HLAP患者入院30 d死亡的AUC分别为0.81、0.67、0.86。CRP、SOFA评分、APACHE Ⅱ评分和sRAGE联合检测鉴别诊断重症HLAP的AUC为0.77。CRP、SOFA评分、APACHE Ⅱ评分、sRAGE和BISAP评分联合检测判断HLAP患者入院30 d死亡的AUC为0.89。结论 sRAGE对HLAP患者病情严重程度的判断有一定意义。联合应用sRAGE和BISAP评分有助于提高对患者短期预后的评估效能。
中图分类号:
汪海平, 李贺. BISAP评分联合血清sRAGE评估急性高脂血症性胰腺炎严重程度和短期预后的价值[J]. 检验医学, 2023, 38(7): 653-658.
WANG Haiping, LI He. BISAP score combined with serum sRAGE for predicting hyperlipidemic acute pancreatitis severity and short-term prognosis[J]. Laboratory Medicine, 2023, 38(7): 653-658.
| 组别 | 例数 | 年龄/岁 | 性别 | BMI/ (kg/m2) | 高血压/ [例(%)] | 糖尿病/ [例(%)] | 动脉氧分压<7.98 kPa/[例(%)] | |
|---|---|---|---|---|---|---|---|---|
| 男/[例(%)] | 女/[例(%)] | |||||||
| 重症组 | 54 | 43.34±9.17 | 40(74.07) | 14(25.93) | 23.75±2.32 | 14(25.93) | 11(20.37) | 15(27.78) |
| 非重症组 | 88 | 40.68±9.54 | 69(78.41) | 19(21.59) | 23.81±2.71 | 17(19.32) | 18(20.45) | 30(34.09) |
| 统计值 | 1.640 | 0.350 | -0.120 | 0.860 | 0.010 | 0.620 | ||
| P值 | 0.100 | 0.550 | 0.910 | 0.350 | 0.990 | 0.430 | ||
表1 重症组和非重症组各项指标比较
| 组别 | 例数 | 年龄/岁 | 性别 | BMI/ (kg/m2) | 高血压/ [例(%)] | 糖尿病/ [例(%)] | 动脉氧分压<7.98 kPa/[例(%)] | |
|---|---|---|---|---|---|---|---|---|
| 男/[例(%)] | 女/[例(%)] | |||||||
| 重症组 | 54 | 43.34±9.17 | 40(74.07) | 14(25.93) | 23.75±2.32 | 14(25.93) | 11(20.37) | 15(27.78) |
| 非重症组 | 88 | 40.68±9.54 | 69(78.41) | 19(21.59) | 23.81±2.71 | 17(19.32) | 18(20.45) | 30(34.09) |
| 统计值 | 1.640 | 0.350 | -0.120 | 0.860 | 0.010 | 0.620 | ||
| P值 | 0.100 | 0.550 | 0.910 | 0.350 | 0.990 | 0.430 | ||
| 组别 | 例数 | 年龄/岁 | 性别 | BMI/ (kg/m2) | 高血压/ [例(%)] | 糖尿病/ [例(%)] | 动脉氧分压<7.98 kPa/[例(%)] | |
|---|---|---|---|---|---|---|---|---|
| 男/[例(%)] | 女/[例(%)] | |||||||
| 死亡组 | 42 | 40.43±9.68 | 32(76.19) | 10(23.81) | 24.01±2.45 | 9(21.43) | 10(23.81) | 14(33.33) |
| 非死亡组 | 100 | 42.44±9.44 | 77(77.00) | 23(23.00) | 23.69±2.62 | 22(22.00) | 19(19.00) | 31(31.00) |
| 统计值 | -1.020 | 0.010 | 0.700 | 0.006 | 0.420 | 0.070 | ||
| P值 | 0.310 | 0.920 | 0.490 | 0.940 | 0.520 | 0.790 | ||
表2 死亡组与非死亡组相关指标比较
| 组别 | 例数 | 年龄/岁 | 性别 | BMI/ (kg/m2) | 高血压/ [例(%)] | 糖尿病/ [例(%)] | 动脉氧分压<7.98 kPa/[例(%)] | |
|---|---|---|---|---|---|---|---|---|
| 男/[例(%)] | 女/[例(%)] | |||||||
| 死亡组 | 42 | 40.43±9.68 | 32(76.19) | 10(23.81) | 24.01±2.45 | 9(21.43) | 10(23.81) | 14(33.33) |
| 非死亡组 | 100 | 42.44±9.44 | 77(77.00) | 23(23.00) | 23.69±2.62 | 22(22.00) | 19(19.00) | 31(31.00) |
| 统计值 | -1.020 | 0.010 | 0.700 | 0.006 | 0.420 | 0.070 | ||
| P值 | 0.310 | 0.920 | 0.490 | 0.940 | 0.520 | 0.790 | ||
| 项目 | β值 | 标准误 | Wald值 | OR值(95%CI) | P值 |
|---|---|---|---|---|---|
| CRP | 0.007 | 0.007 | 1.12 | 1.01(0.99~1.02) | 0.290 |
| APCHE Ⅱ评分 | 0.160 | 0.070 | 3.38 | 1.17(1.03~1.34) | 0.020 |
| SOFA评分 | 0.080 | 0.060 | 1.76 | 1.08(0.96~1.22) | 0.190 |
| sRAGE | 0.005 | 0.002 | 8.20 | 1.01(1.00~1.01) | 0.004 |
表3 重症HLAP的危险因素分析
| 项目 | β值 | 标准误 | Wald值 | OR值(95%CI) | P值 |
|---|---|---|---|---|---|
| CRP | 0.007 | 0.007 | 1.12 | 1.01(0.99~1.02) | 0.290 |
| APCHE Ⅱ评分 | 0.160 | 0.070 | 3.38 | 1.17(1.03~1.34) | 0.020 |
| SOFA评分 | 0.080 | 0.060 | 1.76 | 1.08(0.96~1.22) | 0.190 |
| sRAGE | 0.005 | 0.002 | 8.20 | 1.01(1.00~1.01) | 0.004 |
| 项目 | β值 | 标准误 | Wald值 | OR值(95%CI) | P值 |
|---|---|---|---|---|---|
| CRP | 0.001 | 0.009 | 0.02 | 1.03(0.99~1.05) | 0.070 |
| APCHE Ⅱ评分 | 0.130 | 0.100 | 1.81 | 1.21(0.98~1.32) | 0.090 |
| SOFA评分 | 0.120 | 0.080 | 2.36 | 1.09(0.78~1.32) | 0.440 |
| sRAGE | 0.840 | 0.060 | 8.32 | 1.01(1.00~1.03) | 0.040 |
| BISAP评分 | 1.500 | 0.330 | 21.30 | 1.99(1.53~2.98) | <0.001 |
表4 HLAP患者死亡的多因素分析
| 项目 | β值 | 标准误 | Wald值 | OR值(95%CI) | P值 |
|---|---|---|---|---|---|
| CRP | 0.001 | 0.009 | 0.02 | 1.03(0.99~1.05) | 0.070 |
| APCHE Ⅱ评分 | 0.130 | 0.100 | 1.81 | 1.21(0.98~1.32) | 0.090 |
| SOFA评分 | 0.120 | 0.080 | 2.36 | 1.09(0.78~1.32) | 0.440 |
| sRAGE | 0.840 | 0.060 | 8.32 | 1.01(1.00~1.03) | 0.040 |
| BISAP评分 | 1.500 | 0.330 | 21.30 | 1.99(1.53~2.98) | <0.001 |
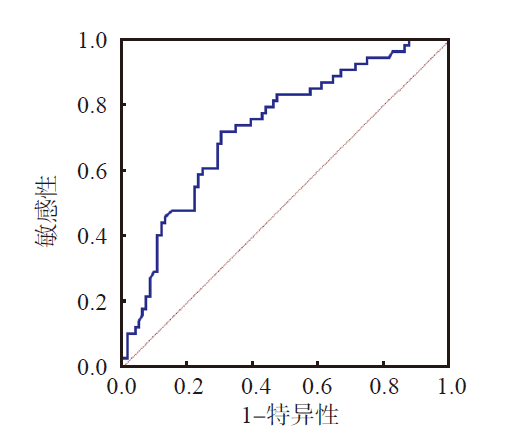
图1 sRAGE鉴别诊断重症HLAP的ROC曲线 注: sRAGE; 参考线。
| 项目 | AUC(95%CI) | 最佳临界值 | 敏感性/% | 特异性/% |
|---|---|---|---|---|
| BISAP评分 | 0.81(0.73~0.87) | 3分 | 78.57 | 72.00 |
| sRAGE | 0.67(0.58~0.74) | 473 pg/mL | 71.43 | 64.00 |
| 联合检测 | 0.86(0.79~0.91) | 0.68 | 83.33 | 76.00 |
表5 BISAP评分、sRAGE单项和联合检测判断HLAP患者入院30 d死亡的效能
| 项目 | AUC(95%CI) | 最佳临界值 | 敏感性/% | 特异性/% |
|---|---|---|---|---|
| BISAP评分 | 0.81(0.73~0.87) | 3分 | 78.57 | 72.00 |
| sRAGE | 0.67(0.58~0.74) | 473 pg/mL | 71.43 | 64.00 |
| 联合检测 | 0.86(0.79~0.91) | 0.68 | 83.33 | 76.00 |

图2 BISAP评分、sRAGE单项和联合检测判断HLAP患者入院30 d死亡的ROC曲线 注: BISAP评分; sRAGE; 联合检测; 参考线。
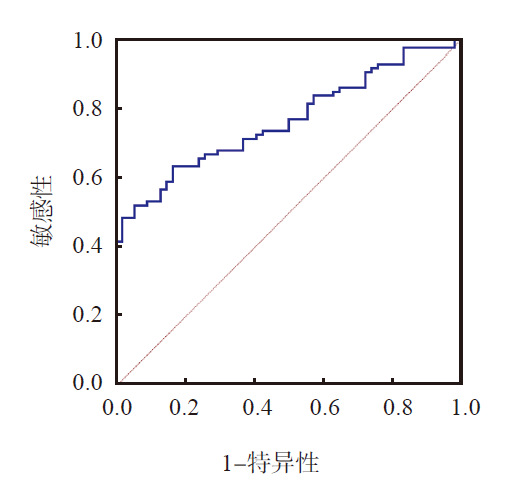
图3 CRP、SOFA评分、APACHE Ⅱ评分和sRAGE联合检测诊断重症HLAP的ROC曲线 注: 联合检测; 参考线。
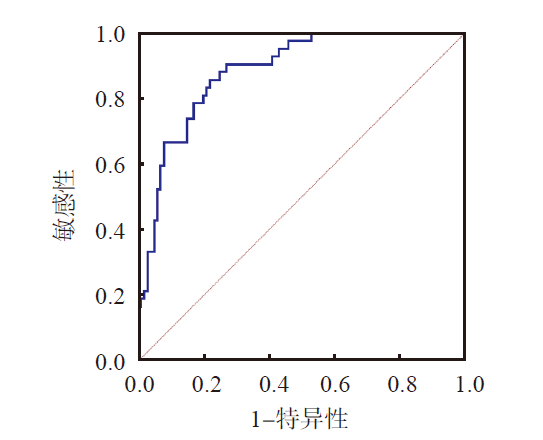
图4 CRP、SOFA评分、APACHE Ⅱ评分、sRAGE和BISAP评分联合检测判断HLAP患者入院30 d死亡的ROC曲线 注: 联合检测; 参考线。
| [1] |
HUANG Y X, JIA L, JIANG S M, et al. Incidence and clinical features of hyperlipidemic acute pancreatitis from Guangdong,China:a retrospective multicenter study[J]. Pancreas, 2014, 43(4):548-552.
DOI URL |
| [2] |
GUBENSEK J, BUTUROVIC-PONIKVAR J, ROMOZI K, et al. Factors affecting outcome in acute hypertriglyceridemic pancreatitis treated with plasma exchange:an observational cohort study[J]. PLoS One, 2014, 9(7):e102748.
DOI URL |
| [3] | WANG Y H, XU Z H, ZHOU Y H, et al. The clinical characteristic of biliary-hyperlipidemic etiologically complex type of acute pancreatitis:a retrospective study from a tertiary center in China[J]. Eur Rev Med Pharmacol Sci, 2021, 25(3):1462-1471. |
| [4] |
HAGJER S, KUMAR N. Evaluation of the BISAP scoring system in prognostication of acute pancreatitis-a prospective observational study[J]. Int J Surg, 2018, 54(Pt A):76-81.
DOI URL |
| [5] |
YANG Y X, LI L. Evaluating the ability of the bedside index for severity of acute pancreatitis score to predict severe acute pancreatitis:a meta-analysis[J]. Med Princ Pract, 2016, 25(2):137-142.
DOI URL |
| [6] |
RAO N L, KOTIAN G B, SHETTY J K, et al. Receptor for advanced glycation end product,organ crosstalk,and pathomechanism targets for comprehensive molecular therapeutics in diabetic ischemic stroke[J]. Biomolecules, 2022, 12(11):1712.
DOI URL |
| [7] |
SHEN X, LI W Q. High-mobility group box 1 protein and its role in severe acute pancreatitis[J]. World J Gastroenterol, 2015, 21(5):1424-1435.
DOI URL |
| [8] |
MAO E Q, TANG Y Q, ZHANG S D. Formalized therapeutic guideline for hyperlipidemic severe acute pancreatitis[J]. World J Gastroenterol, 2003, 9(11):2622-2626.
DOI URL |
| [9] | 中华医学会消化病学分会胰腺疾病学组, 中华胰腺病杂志编辑委员会, 中华消化杂志编辑委员会. 中国急性胰腺炎诊治指南(2013年,上海)[J]. 中华消化杂志, 2013, 33(4):217-222. |
| [10] | HARSHIT KUMAR A, SINGH GRIWAN M. A comparison of APACHE Ⅱ,BISAP,Ranson's score and modified CTSI in predicting the severity of acute pancreatitis based on the 2012 revised Atlanta Classification[J]. Gastroenterol Rep(Oxf), 2018, 6(2):127-131. |
| [11] | TEE Y S, FANG H Y, KUO I M, et al. Serial evaluation of the SOFA score is reliable for predicting mortality in acute severe pancreatitis[J]. Medicine(Baltimore), 2018, 97(7):e9654. |
| [12] |
PARK J Y, JEON T J, HA T H, et al. Bedside index for severity in acute pancreatitis:comparison with other scoring systems in predicting severity and organ failure[J]. Hepatobiliary Pancreat Dis Int, 2013, 12(6):645-650.
DOI URL |
| [13] |
POPA C C, BADIU D C, RUSU O C, et al. Mortality prognostic factors in acute pancreatitis[J]. J Med Life, 2016, 9(4):413-418.
PMID |
| [14] | YANG L, LIU J, XING Y, et al. Comparison of BISAP,Ranson,MCTSI,and APACHE Ⅱ in predicting severity and prognoses of hyperlipidemic acute pancreatitis in Chinese patients[J]. Gastroenterol Res Pract, 2016, 2016:1834256. |
| [15] |
ARIF A, JALEEL F, RASHID K. Accuracy of BISAP score in prediction of severe acute pancreatitis[J]. Pak J Med Sci, 2019, 35(4):1008-1012.
DOI PMID |
| [16] |
LECLERC E, VETTER S W. The role of S100 proteins and their receptor RAGE in pancreatic cancer[J]. Biochim Biophys Acta, 2015, 1852(12):2706-2711.
DOI PMID |
| [17] |
LINDSTRÖM O, TUKIAINEN E, KYLÄNPÄÄ L, et al. Circulating levels of a soluble form of receptor for advanced glycation end products and high-mobility group box chromosomal protein 1 in patients with acute pancreatitis[J]. Pancreas, 2009, 38(8):e215-e220.
DOI URL |
| [18] |
SHAN L, BAI S, ZHAO M. Early diagnosis of serum sICAM-1 and sRAGE in severe acute pancreatitis,and efficacy and prognosis prediction of glutamine combined with ulinastatin[J]. Exp Ther Med, 2021, 21(4):324.
DOI URL |
| [19] | 高莉莎, 王瑞, 任宏飞, 等. 血清可溶性晚期糖基化终产物受体、降钙素原水平预测高脂血症性急性胰腺炎严重程度及预后的临床价值[J]. 实用医院临床杂志, 2021, 18(2):70-73. |
| [20] |
KOCSIS A K, SZABOLCS A, HOFNER P, et al. Plasma concentrations of high-mobility group box protein 1,soluble receptor for advanced glycation end-products and circulating DNA in patients with acute pancreatitis[J]. Pancreatology, 2009, 9(4):383-391.
DOI URL |
| [21] |
ZHAO B, CHEN Y, SUN W W, et al. Effect of S100A12 and soluble receptor for advanced glycation end products on the occurrence of severe acute pancreatitis[J]. J Dig Dis, 2016, 17(7):475-482.
DOI URL |
| [22] |
HUDSON B I, GARDENER H, LIU-MARES W, et al. Serum soluble RAGE levels and carotid atherosclerosis:the Northern Manhattan Study(NOMAS)[J]. Atherosclerosis, 2015, 240(1):17-20.
DOI URL |
| [23] |
BRODSKA H, MALICKOVA K, VALENTA J, et al. Soluble receptor for advanced glycation end products predicts 28-day mortality in critically ill patients with sepsis[J]. Scand J Clin Lab Invest, 2013, 73(8):650-660.
DOI PMID |
| [1] | 史健, 雷静, 耿燕. 宏基因组二代测序在肺部感染诊断中的应用价值[J]. 检验医学, 2025, 40(12): 1232-1236. |
| [2] | 袁昳玮, 王艺文, 费张莉, 黄湾. 基于炎症指标构建抗MDA5抗体阳性皮肌炎合并间质性肺炎患者预后不良风险评估模型[J]. 检验医学, 2025, 40(9): 841-847. |
| [3] | 郭漫漫, 张鹏, 王润智, 史珑. 血清lncRNA NEAT1和miR-29c-3p表达与癫痫患儿病情及预后的相关性[J]. 检验医学, 2025, 40(8): 763-768. |
| [4] | 王小波. 167 202例临床样本抗核抗体检测结果回顾性分析[J]. 检验医学, 2025, 40(6): 583-591. |
| [5] | 施方静, 胡姗姗, 罗信国, 朱艳, 俞方泉, 叶虹位. 慢性淋巴细胞白血病患者程序性死亡分子1/程序性死亡-配体1的表达及其临床意义[J]. 检验医学, 2025, 40(6): 592-595. |
| [6] | 陈晓艳, 莫倩儿, 黄方滢, 胡子鹏, 杨珊珊, 农菁菁, 杨雪丽. 基于高通量测序技术分析多发性硬化症患者TCR图谱特征[J]. 检验医学, 2025, 40(5): 421-427. |
| [7] | 杜笑青, 石丽平, 周梦, 姚丽敏. 寻常型银屑病患者外周血IFN-γ、IL-4、Hcy水平与颈动脉粥样硬化的关系[J]. 检验医学, 2025, 40(4): 388-392. |
| [8] | 李汉华, 吴亚洲, 翁文浩. 自身免疫性脑炎相关抗体实验室检测现状[J]. 检验医学, 2025, 40(3): 209-217. |
| [9] | 马展, 翁文浩. 儿童自身免疫性肝病及其实验室诊断进展[J]. 检验医学, 2025, 40(3): 218-222. |
| [10] | 张燕, 郑洁, 刘佳星, 高硕, 徐学静, 刘畅, 曹小利, 周万青, 沈瀚. 免疫功能正常肺隐球菌病患者隐球菌荚膜抗原检测的意义[J]. 检验医学, 2024, 39(12): 1157-1162. |
| [11] | 刘国利, 王颖, 王莹, 段旭东, 金花. 卵巢上皮性肿瘤患者贝伐单抗治疗后血脂水平变化及其对预后的影响[J]. 检验医学, 2024, 39(12): 1196-1201. |
| [12] | 王瑛, 张颐豪, 季玮, 付燕, 于雪莹, 张慧, 胡婷婷, 沈薇, 满秋红. 抗U1-RNP抗体和抗RNPA/RNP68抗体联合检测在自身免疫性疾病诊断中的价值[J]. 检验医学, 2024, 39(11): 1066-1071. |
| [13] | 胡传玺, 刘灵燕, 李漫. 间接免疫荧光法、线性免疫印迹法、化学发光法单项和联合检测抗核抗体的临床价值[J]. 检验医学, 2024, 39(11): 1072-1077. |
| [14] | 张勤, 姚瀚鑫, 王伯玉, 巨昕薇, 续薇. t-PSA及其衍生指标PHI和PI-RADS评分对前列腺癌诊断效能的评价[J]. 检验医学, 2024, 39(11): 1084-1090. |
| [15] | 蒙强, 王双, 白舟, 黄茜, 付阳. 红细胞膜表面TLR9表达在脓毒症相关性贫血中的临床价值[J]. 检验医学, 2024, 39(10): 933-938. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
