检验医学 ›› 2015, Vol. 30 ›› Issue (10): 987-990.DOI: 10.3969/j.issn.1673-8640.2015.10.005
李多孚1, 陈郁琳2, 夏雨3
LI Duofu1, CHEN Yulin2, XIA Yu3
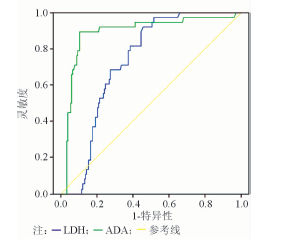
摘要: 探讨胸水中腺苷脱氨酶(ADA)、乳酸脱氢酶(LDH)对鉴别结核性、癌性和其它疾病胸腔积液的临床价值。 回顾性分析行胸腔积液常规检测的住院患者的资料,其中结核患者38例、肿瘤患者74例、其它疾病患者108例。应用受试者工作特征(ROC)曲线确定胸腔积液ADA、LDH诊断结核性胸膜炎的最佳临界值,并计算ADA、LDH诊断结核性胸膜炎的临床诊断效能。 结核组、肿瘤组、其它疾病组ADA活性{中位数(M)[四分位间距(Q)]}分别为47.30(26.50)、8.15(6.50)、5.40(8.40)U/L,各组间差异均有统计学意义(Z值分别为6.981、6.978、2.302,P均<0.05);LDH活性[M(Q)]分别为453.68(242.07)、252.00(368.00)、101.50(192.00)U/L,各组间差异均有统计学意义(Z值分别为2.419、5.386、4.324,P均<0.05)。ROC曲线确定胸腔积液ADA诊断结核性胸膜炎的最佳临界值为26.7 U/L,灵敏度为89.5%、特异性为89.6%;LDH诊断结核性胸膜炎的最佳临界值为173.5 U/L,灵敏度为92.1%、特异性为54.4%;ADA和LDH联合检测的灵敏度为89.5%、特异性为54.1%。 胸腔积液ADA是诊断与鉴别结核性胸膜炎重要的指标,LDH特异性相对较低,但也有一定的参考意义。两者联合检测的临床诊断效能并不升高。
中图分类号: